Loading...
5.4-5.5 Muscle and Nervous Tissues Identification Practice
Quiz by Cathy Schopf
Customize this quiz to suit your class
Instantly translate to 100+ languages
Tag the questions with any skills you have. Your dashboard will track each student's mastery of each skill.
Give this quiz to my class
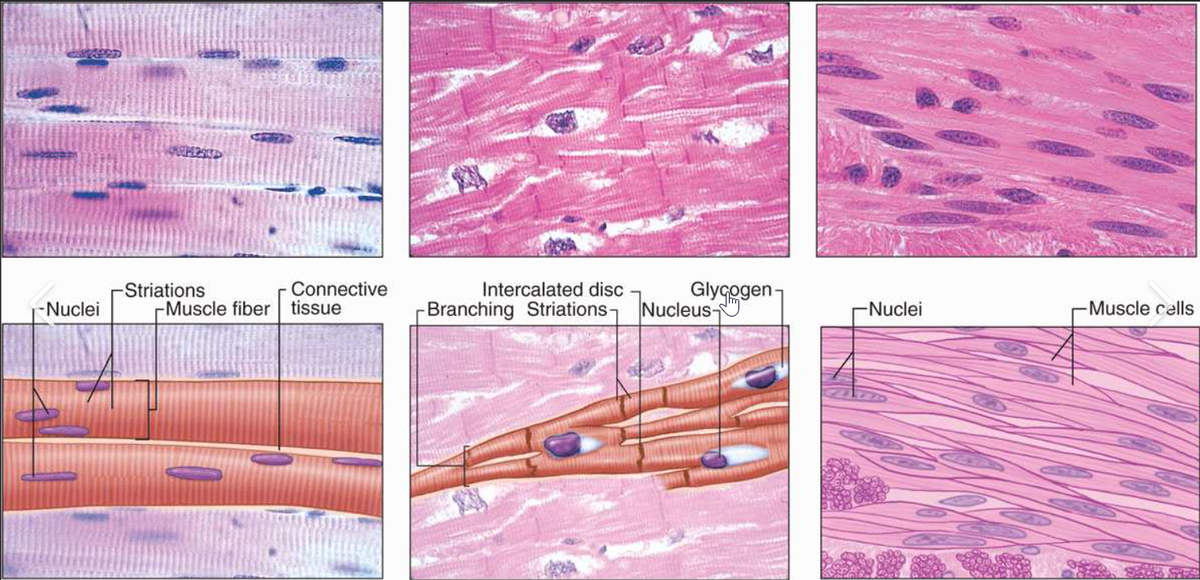
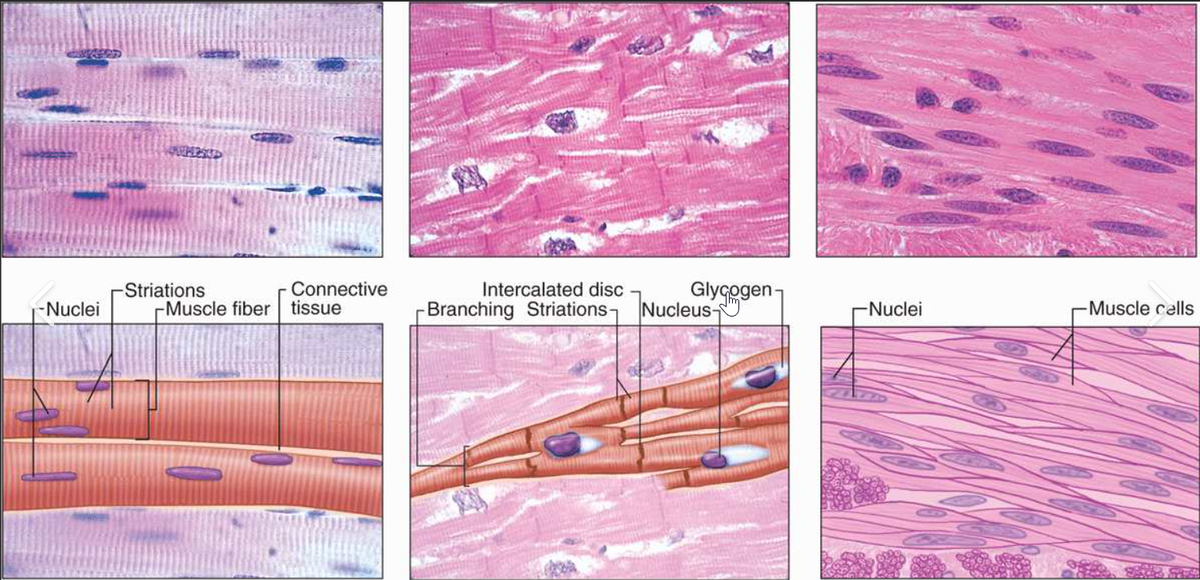
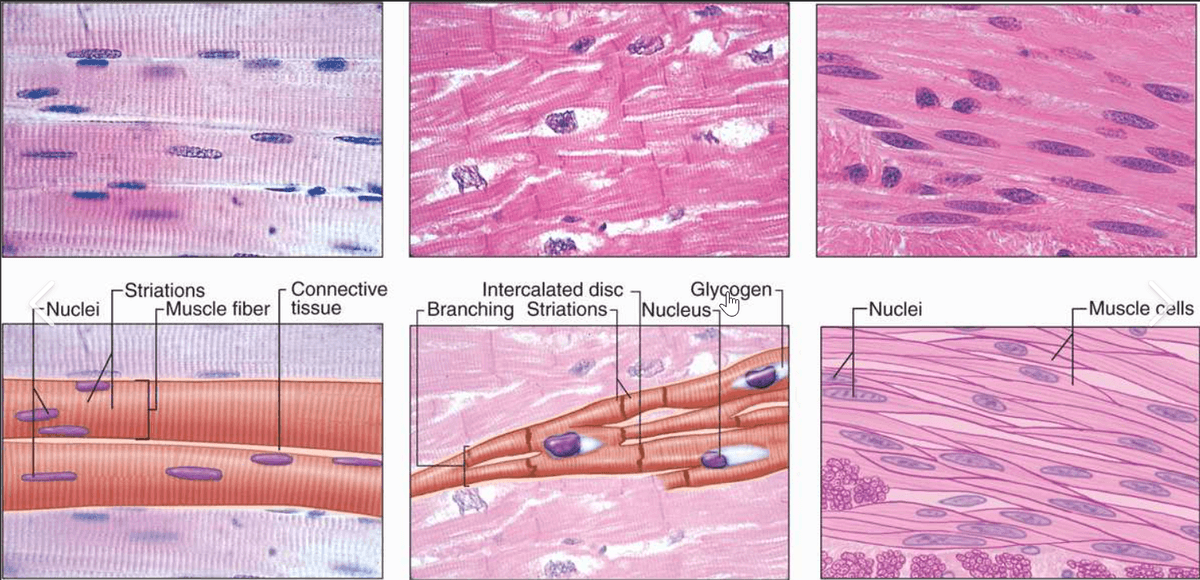
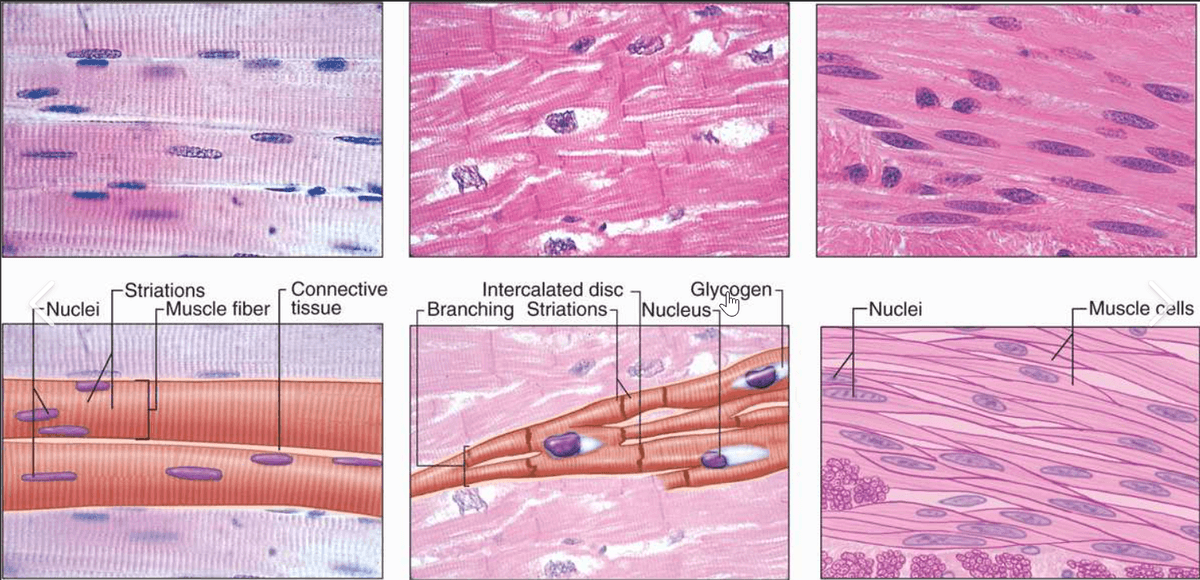
Which type of muscle tissue is shown on the left?
nervous tissue
skeletal muscle tissue
smooth muscle tissue
cardiac muscle tissue
Which type of muscle tissue is shown in the middle?
smooth muscle tissue
nervous tissue
cardiac muscle tissue
skeletal muscle tissue
Which type of muscle tissue is shown on the left?
Which type of muscle tissue is shown in the middle?
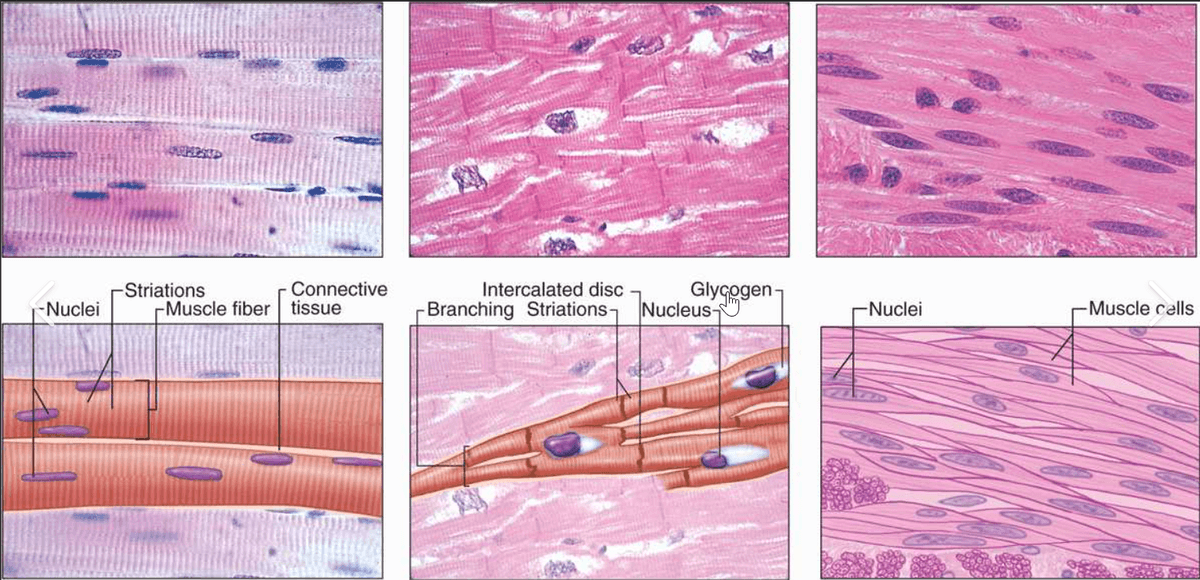
Which muscle tissue is shown on the right?
Which image shows cardiac muscle tissue?
Which image shows smooth muscle tissue?
Which image shows skeletal muscle tissue?
Which property of muscle tissue means that the cells can shorten?
Which type of muscle tissue is NOT striated?
Which muscle tissue is VOLUNTARY?
Which muscle tissue has many nuclei in each cell?
Which image shows nervous tissue?
What important function does nervous tissue do for our bodies?