Loading...
Cardiology Board Review
Quiz by Shyam Raja
Tag the questions with any skills you have. Your dashboard will track each student's mastery of each skill.
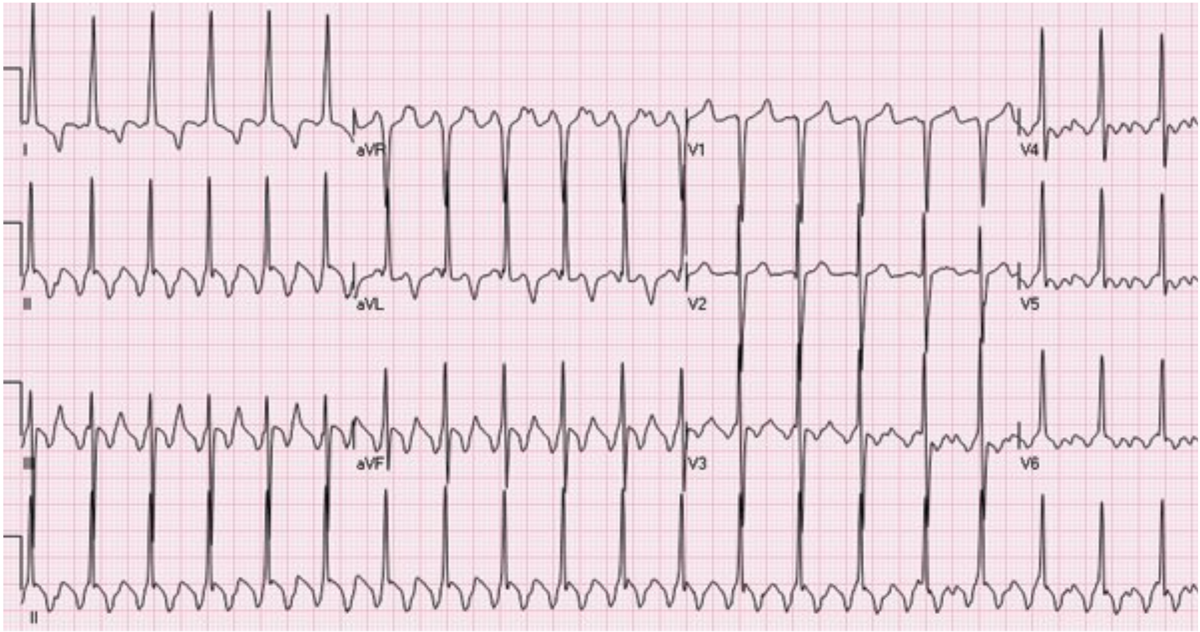
A 56-year-old man is evaluated in the emergency department for acute shortness of breath and the sensation of a racing heart. His only medical problem is hypertension treated with chlorthalidone.
On physical examination, blood pressure is 89/52 mm Hg and pulse rate is 150/min. Cardiac examination reveals a regular tachycardia. Jugular venous distention and pulmonary crackles are present.
ECG is shown. The patient is successfully cardioverted.
Which of the following is the most appropriate additional treatment?
Flecainide
No Additional Treatment
Amiodarone
Metoprolol
Catheter Ablation
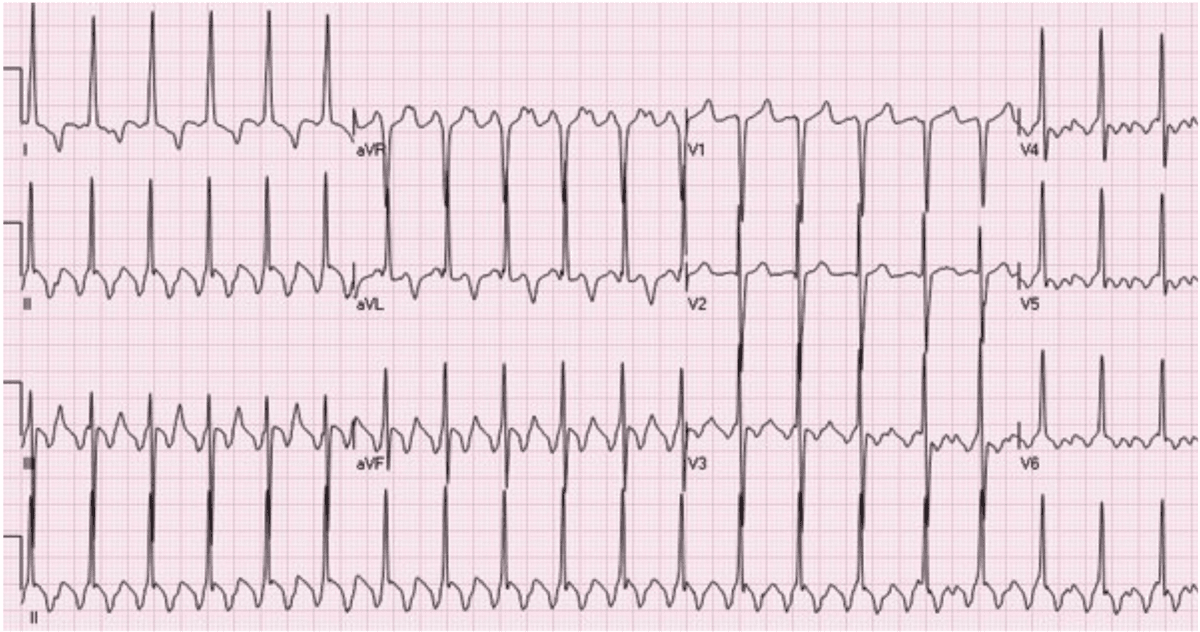
A 56-year-old man is evaluated in the emergency department for acute shortness of breath and the sensation of a racing heart. His only medical problem is hypertension treated with chlorthalidone.
On physical examination, blood pressure is 89/52 mm Hg and pulse rate is 150/min. Cardiac examination reveals a regular tachycardia. Jugular venous distention and pulmonary crackles are present.
ECG is shown. The patient is successfully cardioverted.
Which of the following is the most appropriate additional treatment?
A 68-year-old man is evaluated 1 month after atherectomy and stenting of the right superficial femoral artery for severe claudication. Since the procedure, he can walk and perform all of his customary activities without claudication. Medical history is significant for hypertension, hyperlipidemia, and coronary artery disease. He exercises 150 minutes weekly and consumes a heart-healthy diet. He quit smoking 15 years ago. Medications are low-dose aspirin, low-dose rivaroxaban, metoprolol, ramipril, and high-intensity rosuvastatin.
On physical examination, blood pressure is 124/70 mm Hg. The remainder of the physical examination is unremarkable.
Laboratory studies reveal a serum total cholesterol level of 120 mg/dL (3.1 mmol/L), serum LDL cholesterol level of 50 mg/dL (1.3 mmol/L), and serum HDL cholesterol level of 48 mg/dL (1.2 mmol/L).
Which of the following is the most appropriate additional treatment?
A 47-year-old man is evaluated for a heart murmur. He is asymptomatic and has no exercise limitations.
On physical examination, vital signs, including blood pressure, are normal. There is a grade 1/6 decrescendo diastolic murmur heard at the left sternal border. The remainder of the examination is normal.
Echocardiogram shows a left ventricular ejection fraction of 55%, a bicuspid aortic valve with mild aortic regurgitation, and a normal left ventricular end-systolic dimension. The ascending aorta is enlarged, with a dimension of 4.2 cm. Echocardiographic imaging quality of the aortic sinuses, sinotubular junction, and ascending aorta is excellent.
Which of the following is the most appropriate management?
A 48-year-old man is evaluated for recurrent pericarditis. Six months ago, he had acute pericarditis treated with ibuprofen and colchicine. His symptoms resolved completely within 3 weeks of initiation of therapy. Evaluations for an infectious cause and connective tissue disease were negative. The patient's symptoms recurred after ibuprofen was tapered over 1 month with continuation of colchicine. Ibuprofen was re-initiated at a high dose with resolution of symptoms and tapered over a 2-month period. His current symptoms began 24 hours ago. Currently, his only medication is colchicine.
On physical examination, temperature is 38.0 °C (100.4 °F); other vital signs are normal. Pulsus paradoxus of 10 mm Hg is present. There is no jugular venous distention. The lungs are clear to auscultation. A friction rub is heard at the left sternal border and apex.
ECG shows normal sinus rhythm with widespread ST-segment elevation of 0.5 to 1.0 mm. Echocardiogram shows a small circumferential pericardial effusion (diastolic echo-free space, 3 mm) without evidence of tamponade.
Which of the following is the most appropriate treatment?
A 60-year-old woman comes to the office for follow-up evaluation 1 year after having a drug-eluting stent placed in the mid left anterior descending coronary artery to treat non–ST-elevation acute coronary syndrome. She has been adherent to dual antiplatelet therapy for the past year without any bleeding events. The patient's only other medical problem is diabetes mellitus. Medications are metformin, liraglutide, atorvastatin, clopidogrel, and aspirin.
Which of the following is the most reasonable management of the antiplatelet therapy?
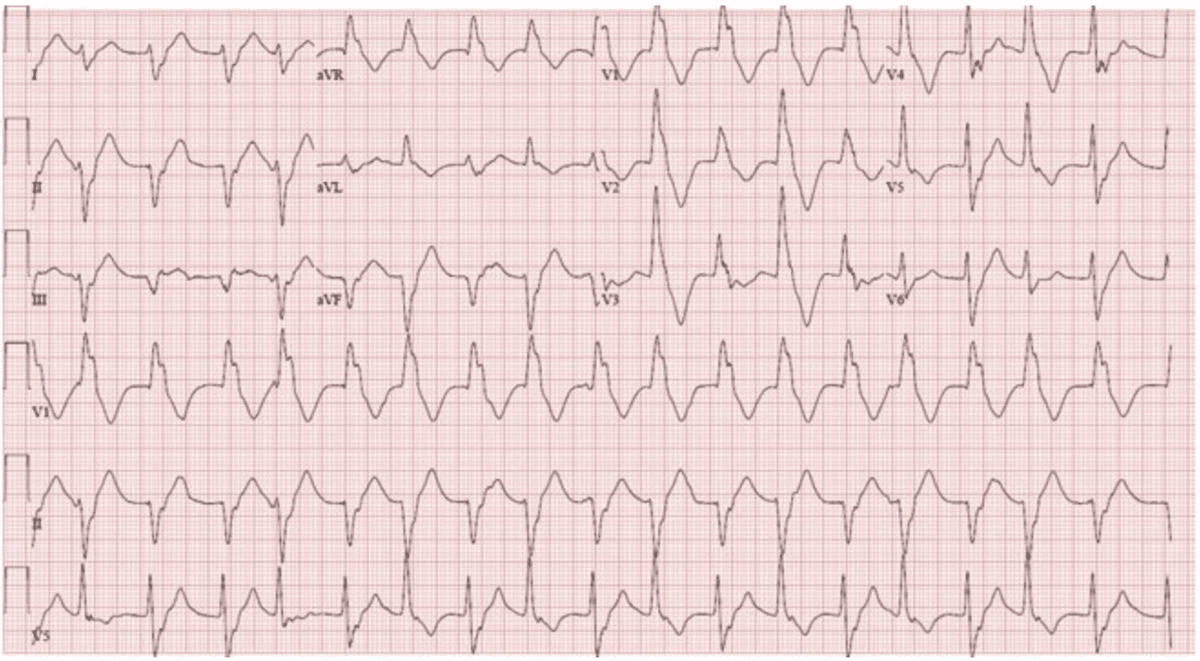
A 61-year-old man is evaluated in the emergency department for palpitations that began this morning. He has a history of coronary artery disease treated with coronary artery stenting 18 months ago and left ventricular dysfunction. Medications are aspirin, metoprolol, spironolactone, and lisinopril.
On physical examination, blood pressure is 100/65 mm Hg and pulse rate is 130/min; other vital signs are normal. Oxygen saturation is 98% with the patient breathing ambient air. Intermittent cannon a waves are noted on neck examination. Other than tachycardia, cardiac examination is normal. Breath sounds are clear.
ECG with rhythm strips is shown.
Which of the following is the most likely diagnosis?
A 47-year-old man is evaluated for management of heart failure with reduced ejection fraction (ejection fraction, 30%) diagnosed 3 years ago. He has New York Heart Association functional class III symptoms and has been stable for the past year. His medical history also includes ACE inhibitor–induced angioedema, spironolactone-induced gynecomastia, and atrial fibrillation. An implantable cardioverter-defibrillator is in place. Medications are losartan, carvedilol, empagliflozin, furosemide, and apixaban.
On physical examination, blood pressure is 120/68 mm Hg and pulse rate is 78/min and irregular. Other than an irregularly irregular heart rhythm, the remainder of the examination is normal.
Serum creatinine and electrolyte levels are normal.
Which of the following is the most appropriate treatment?
A 45-year-old man is seen for cardiovascular risk reduction. Hyperlipidemia was diagnosed 4 years ago and is treated with atorvastatin. He has a 35-pack-year history of cigarette smoking and is a current smoker. Six months ago, prediabetes was diagnosed. He occasionally has a depressed mood. He does not take aspirin on a regular basis.
On physical examination, vital signs are normal. BMI is 29. The remainder of the examination is unremarkable.
Which of the following is the most appropriate management?
A 56-year-old woman is evaluated before starting treatment with trastuzumab for early-stage HER2-positive breast cancer. She has no cardiovascular symptoms and has no exercise-related limitations. She has hypertension and hyperlipidemia. Medications are losartan and atorvastatin.
On physical examination, vital signs and other findings are normal. The breast surgery site has healed.
Results of routine laboratory studies are normal.
Findings on echocardiogram are normal. Left ventricular ejection fraction is 55%.
Which of the following is the most appropriate cardiac surveillance for this patient?
A 69-year-old man is evaluated for persistent angina despite maximally tolerated antianginal therapy. Symptoms appear after walking less than one-half mile and interfere with his quality of life and occupation as a mail carrier. He has no pain at rest or heart failure symptoms. He frequently experiences light-headedness when arising from a seated position. He has a 20-pack-year history of smoking but stopped 25 years ago. Medications are aspirin, metoprolol, sublingual nitroglycerin, and rosuvastatin.
On physical examination, blood pressure is 108/72 mm Hg, pulse rate is 54/min, and respiration rate is 20/min. The remainder of the physical examination is normal.
An ECG shows sinus rhythm. A chest radiograph is normal.
Which of the following is the most appropriate management?
A 70-year-old man is referred for evaluation after a 6.1-cm abdominal aortic aneurysm was discovered on routine screening ultrasonography. Medical history is significant for hypertension and hyperlipidemia. He has a 50-pack-year history of cigarette smoking, stopping 6 years ago. Medications are rosuvastatin and chlorthalidone.
On physical examination, vital signs are normal. BMI is 28. A bruit is heard over the abdomen, and a pulsatile abdominal mass is present to the left of the midline.
Which of the following is the most appropriate next step in management?
A 55-year-old woman is evaluated for a 6-month history of progressive fatigue and dyspnea while walking on level ground.
On physical examination, blood pressure is normal and pulse rate is 80/min. Cardiac examination reveals an opening snap and a diastolic rumble heard best at the cardiac apex. Estimated central venous pressure is normal.
A resting echocardiogram shows a left ventricular ejection fraction greater than 55% and a normal-size right ventricle with preserved function. The mitral valve is thickened and appears rheumatic, with restricted opening of the leaflet tips. The mitral gradient and calculated valve area are consistent with moderate mitral stenosis.
Which of the following is the most appropriate management?
A 74-year-old man is evaluated in the emergency department for somnolence. He resides in a skilled nursing facility. His transfer note indicates that he has moderately severe Alzheimer disease treated with donepezil.
On physical examination, blood pressure is 70/40 mm Hg and pulse rate is 30/min; other vital signs are normal. Oxygen saturation with the patient breathing ambient air is 97%. The patient is difficult to arouse. Cardiac examination reveals bradycardia but is otherwise unremarkable.
Complete blood count and electrolyte levels are normal.
Cardiac telemetry shows sinus bradycardia with heart rate of 30/min.
Which of the following is the most appropriate treatment?
A 78-year-old woman is evaluated for a 3-month history of heart failure with reduced ejection fraction (ejection fraction, 20%). She has stable dyspnea when walking up stairs but has no other symptoms. Her medical history is otherwise unremarkable. Medications are valsartan-sacubitril, carvedilol, furosemide, empagliflozin, and spironolactone. Carvedilol is at half-maximum dosage; all other medications are at maximum recommended dosages.
On physical examination, blood pressure is 118/74 mm Hg and pulse rate is 88/min. BMI is 27, unchanged from her last visit. Central venous pressure and the remainder of the examination are normal.
Which of the following is the most appropriate treatment?