Loading...
Muscles and Muscle Actions
Quiz by Zachary P Tuschen
Customize this quiz to suit your class
Instantly translate to 100+ languages
Tag the questions with any skills you have. Your dashboard will track each student's mastery of each skill.
Give this quiz to my class
What is muscle A?
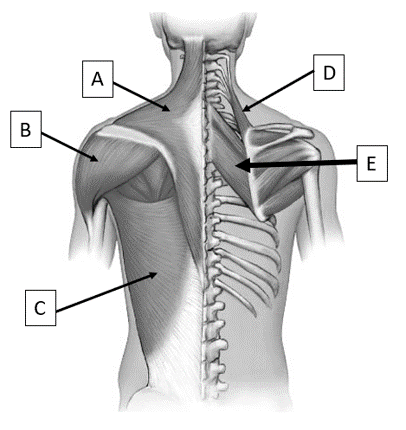
Levator scapulae
Rhomboids
Trapezius
Latissimus dorsi
Deltoid
Zygomaticus
What is muscle B?
Rhomboids
Trapezius
Latissimus dorsi
Zygomaticus
Levator scapulae
Deltoid
What is muscle A?
What is muscle B?
What is muscle C?
What is muscle D?
What is muscle E?
What is the action of muscle A?
What is the action of muscle E?
What is the action of muscle B?
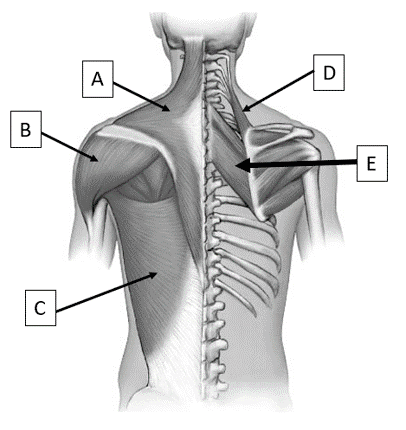
What is muscle A?
What is muscle B?
What is muscle C?
What is muscle D?
What muscle in the image has a large role in allowing you to cross your legs?
What muscle in the image performs hip adduction?
What muscle in the image performs hip extension?
What is muscle A in the image?

What is muscle B in the image?
What muscle in the image is used to perform flexion of the wrist?
What muscle in the image is used to perform wrist extension?
What muscle in the image is responsible for elbow extension?

What muscle performs shoulder abduction?
The gastrocnemius and soleus connect to the heel bone via which tendon?
Which muscles attach to the tibial tuberosity via the patellar tendon?
The hamstrings consist of how muscles?