Loading...
PH Sistem Gerak
Quiz by ANISA PUTERI
Customize this quiz to suit your class
Instantly translate to 100+ languages
Tag the questions with any skills you have. Your dashboard will track each student's mastery of each skill.
Give this quiz to my class
Identifikasikanlah tulang tulang berdasarkan jenisnya !
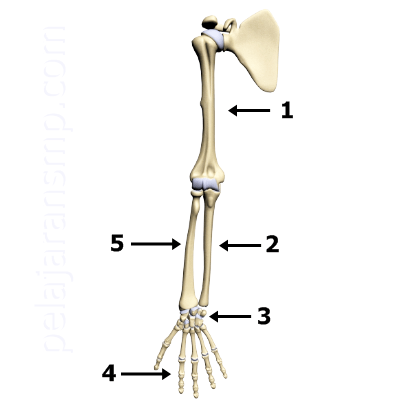
Identifikasikanlah tulang tulang tersebut berdasarkan nomor dan nama tulangnya !
Identifikasikanlah tulang tulang berdasarkan jenisnya !
Identifikasikanlah tulang tulang tersebut berdasarkan nomor dan nama tulangnya !

Tulang merupakan tulang gerak pasif karena ....
Rangka dapat memberi bentuk tubuh manusia
Rangka adalah tempat melekatnya otot dalam tubuh manusia
Rangka menjadi sebuah tempat mengaturnya pergerakan sendi dan otot
Rangka dapat melindungi organ yang terdapat dalam tubuh manusia
Rangka akan meregenarasi sel dari sumsum tulang
Organ yang tersusun atas tulang rawan diantaranya ....