Loading...
Practical English 3 & Unit 6A Homework
Quiz by Borys Perchenko
Customize this quiz to suit your class
Instantly translate to 100+ languages
Tag the questions with any skills you have. Your dashboard will track each student's mastery of each skill.
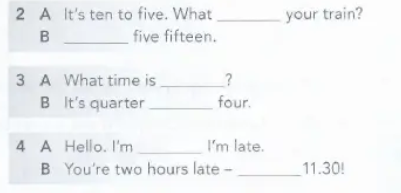
Fill in the gaps. Вставте пропуски.
Listen to the audio and choose the right options. Послухайте аудіо і оберіть правильні відповіді.
Fill in the gaps. Вставте пропуски.

Listen to the audio and choose the right options. Послухайте аудіо і оберіть правильні відповіді.
Give this quiz to my class