Loading...
SM's L3 Questions
Quiz by Tonisha Ambrose
Tag the questions with any skills you have. Your dashboard will track each student's mastery of each skill.
What are 3 possible Histories or Pathologies that you could have to indicate a CCTA workup?
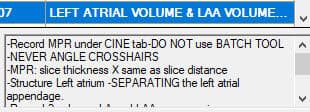
EP Trunk Lengths need to be done in PA.
What are 3 possible Histories or Pathologies that you could have to indicate a CCTA workup?

EP Trunk Lengths need to be done in PA.
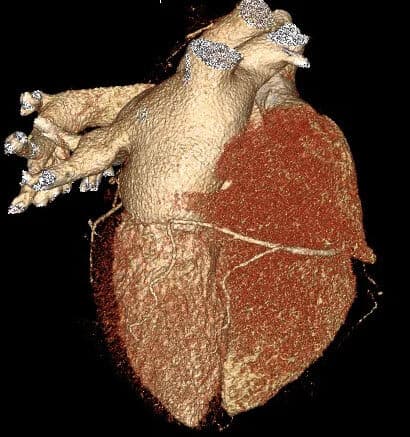
Which is a correct way to start a VRT TREE LR spin?

What are the 4 Chambers of the Heart?

What vessel(s) most commonly come off the RT Coronary Cusp?

What is the first part of the vessel of the called that comes off the LT Coronary Cusp?
A PDA/PLA can only come off one side of the heart.

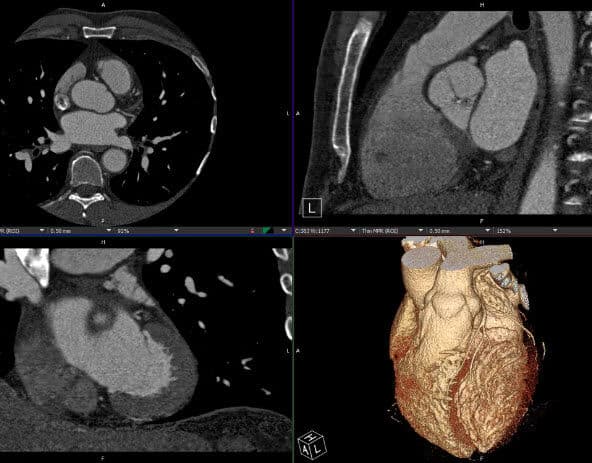
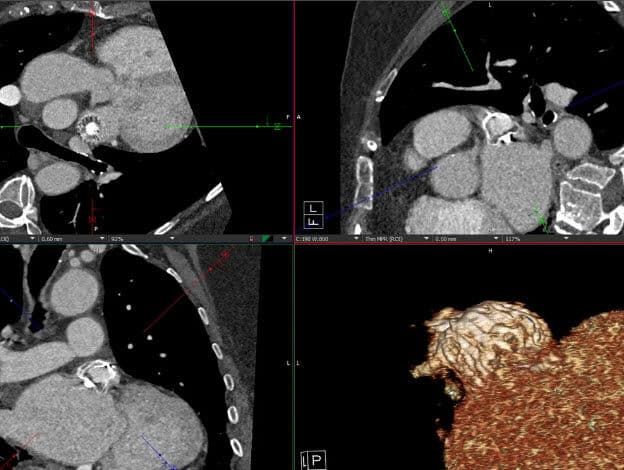
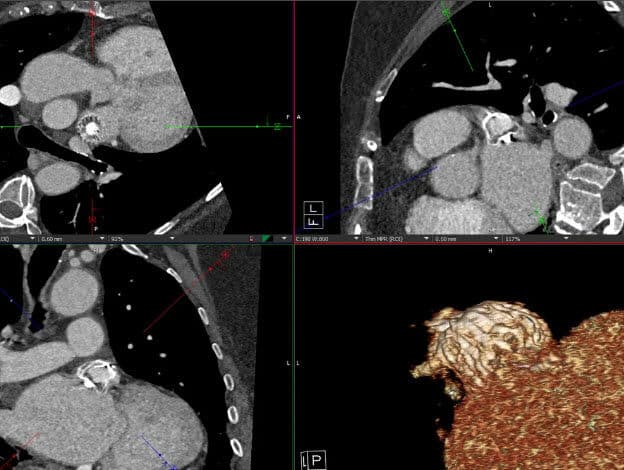
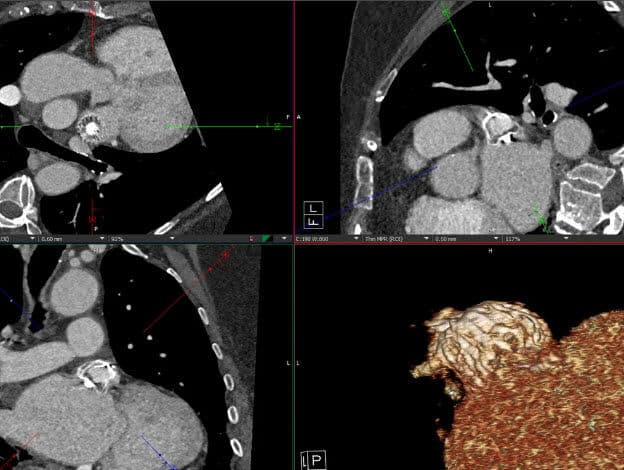
What MPR do you line up with the Mitral Valve and the Aortic Valve?

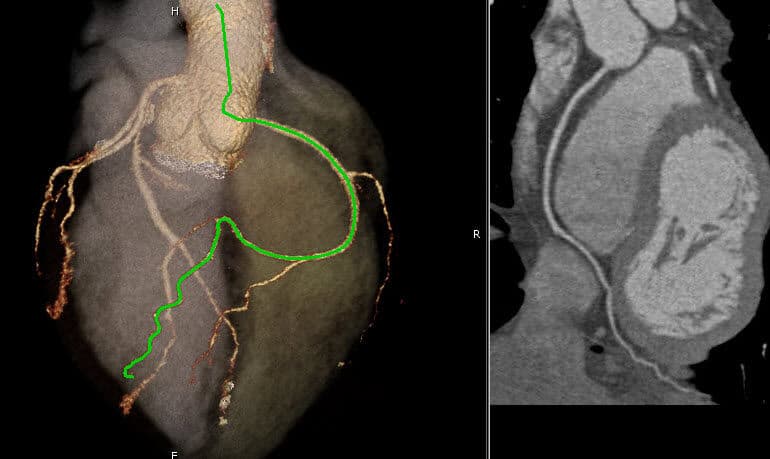
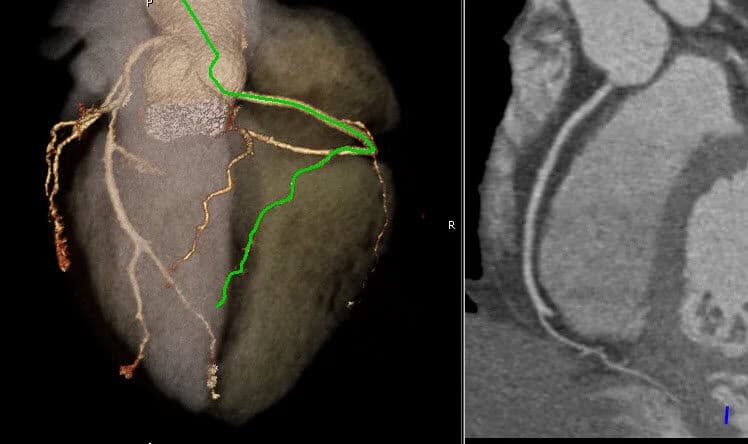
Which CPR comes off the LT Coronary Cusp and goes to the front following the interventricular groove?

You can have multiple AMs, OMs, and D1s and you spin them all.

Where does a PLA end up?
Can you have a RCA, RCA/PLA, and a RCA/PDA on the same scan?
Where does the PDA end up?
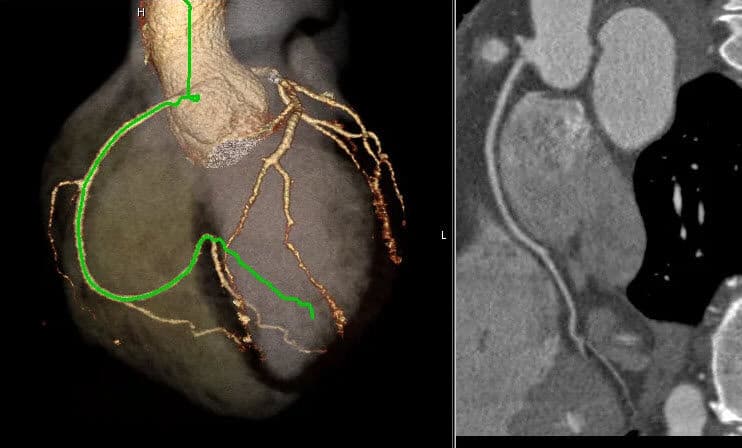
What vessel(s) come off the RCA?

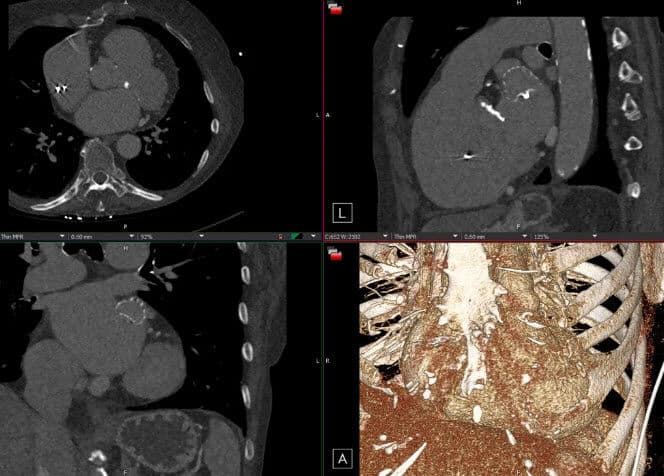
What are the main MPRs that you do for a CCTA protocol?

You will always have a heart shadow on tera.

You never have to check other phases or plot additional CPRs?

What is different about Kettering CPRs?

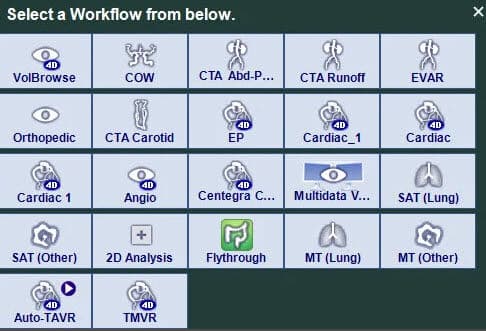
What workflow do you use to load a CCTA on tera?
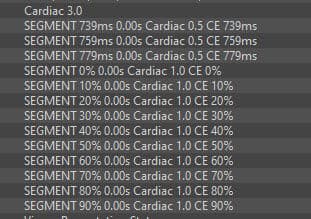
How do you click through the percentages on tera?

The preloaded MPRs are always correct.

You always spin a CPR in vertical?

What is your favorite protocol? Visage or Tera?
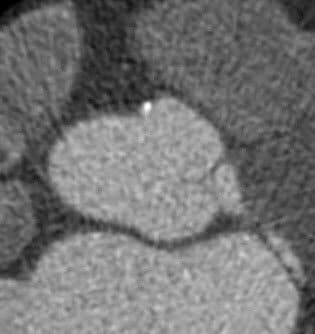
Are Calcium Scores Contrasted? What thickness should they be?

On Calcium Scores, you should leave the tinting ON, unless specifically stated otherwise?

If there is calcium in the valve, you should still score it?

Do you score the entire vessel or just the origin?

Calcium Scores and Calcium Valve Scores are the same thing?
You should score stents and clips.

You will always have a Ramus.

You have a true RCA, can you also have an RCA/PDA?
Do you have to always score an OM?

When sent, you should ALWAYS reference the contrasted images to help you determine where the calcium is.
You must score all calcium that is present from the origin of the vessel to the tip. Never include the valve.

Spin the longest, most dominant accessory vessel (AM, D1, OM).

The higher the score on the calcium score means a higher likelihood of CAD. This is why we must provide accurate scores.

Coreline is an AI software that selects the calcium for you. You only need to verify that the vessels scored correctly.

Calcium Scores can be scored on Visage, Tera, Vitrea and Coreline.

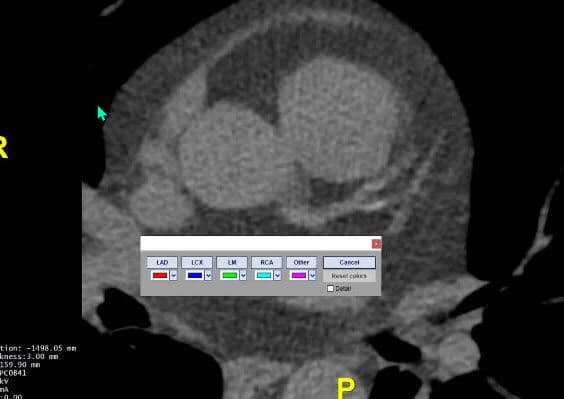
Do you use 'other' to score vessels on tera?
Do you score stents, grafts, or clips along with the vessel?

What does a CFA evaluate?
When are the ventricles the smallest?

When are the ventricles the largest?

Anytime we receive CCTA, CFA, CA+ Score images, we should process all 3 protocols.
If the phases are out of order, where do you need to send it first to process it?

Gating the scan shows the heart beating, allowing for visualization of the left ventricle pumping out the blood.

If the case is routine, you must pick up all three protocols- CCTA, CA+ Score and the CFA.
What are the 4-Chambers of the heart?
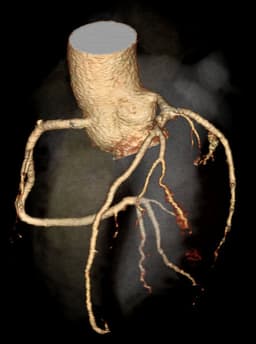
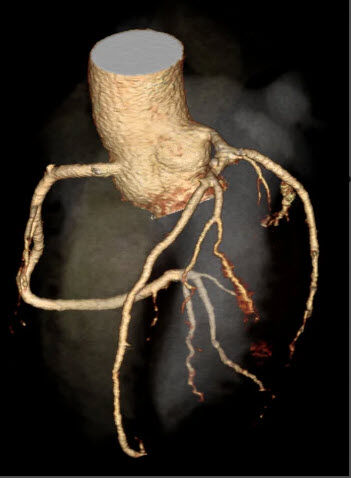
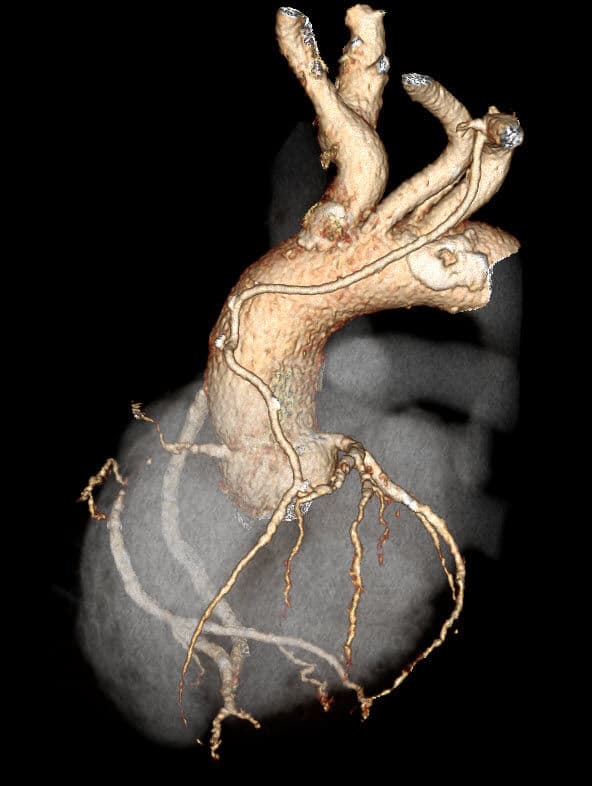
What do you EP's evaluate?

What are 3 histories for EP Planning?

For EP's the best phase to use is typically what?

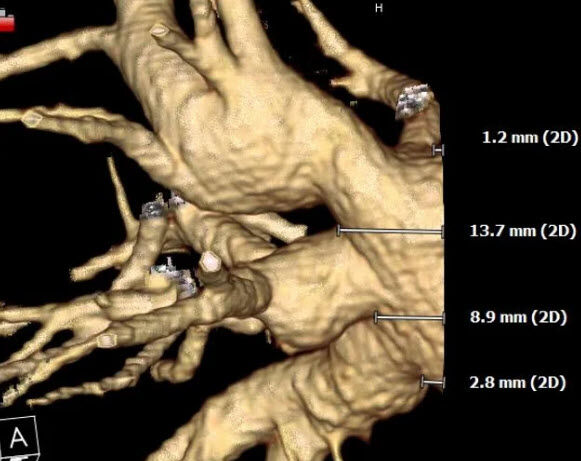
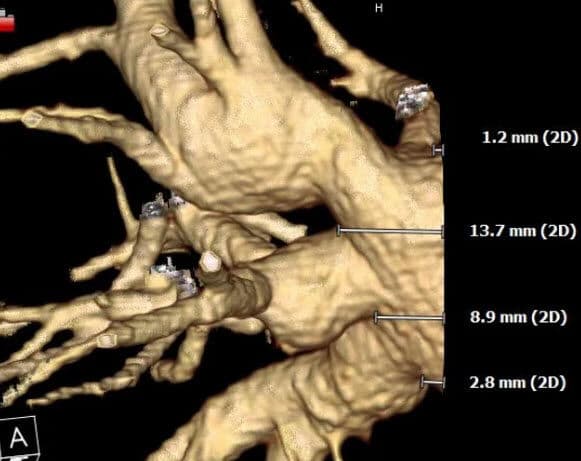
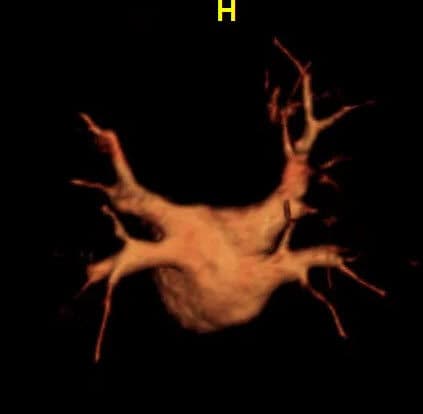
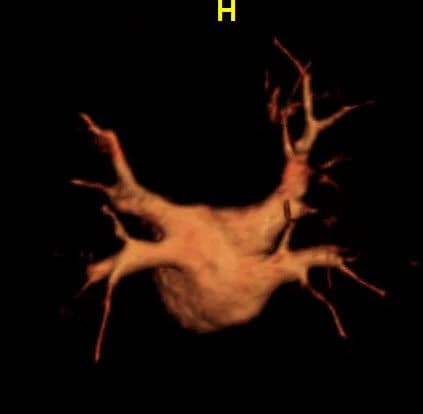
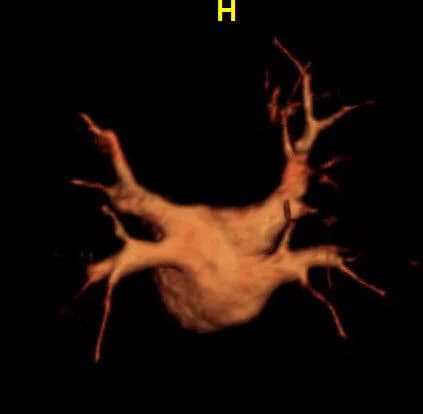
What are the branches named that you measure?

The volume for an EP is spun in AP and LR most of the time.

When loading an EP, it is correct to use the cardiac_1 workflow.

When doing your volume for an EP, what must be included?

Does the EP volume start in AP?
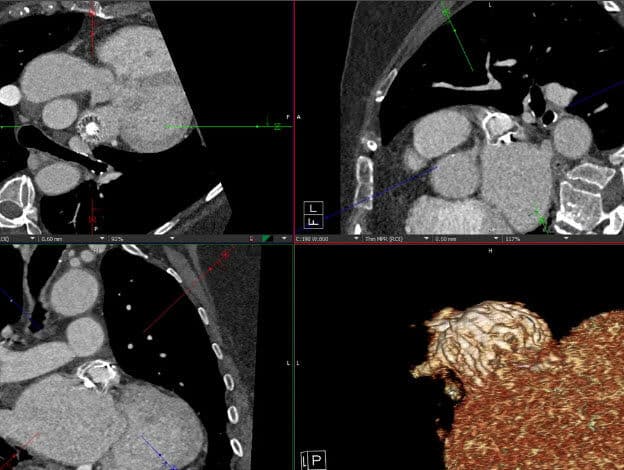
The ostium to first branch on TERA is done on what?

Do MRA EPs have any MPRs?
What do you need to do for MRAs when they send over a bunch of series?

Since the MRA EP Volume is almost done for you, what do you want to cut off?
Do you still have to move the white line down under the 3D Color Map for a MRA EP?
Are the EP MRA measurements exactly like doing measurements on visage?
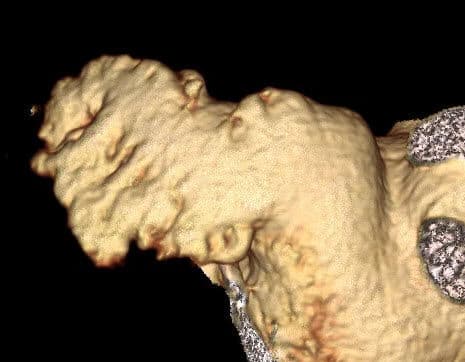
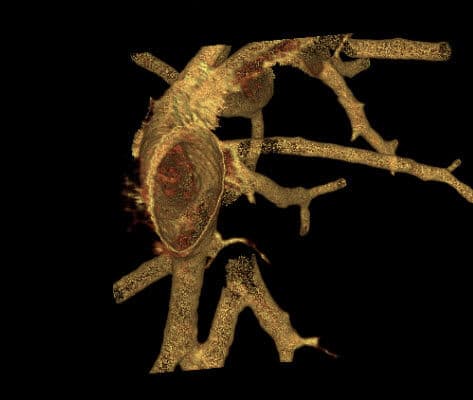
What is a Watchman's device?
How does a watchman's device work?

There are Measurements on the Post LAA.

If there are delayed images sent, then you must provide MPRs for every protocol.

When an EP and a LAA Pre-Op are ordered on the same patient, you must do the delayed series for both protocols.
What is included in the volume for the Post LAA?
What are the two snapshots you have to take (when protocol says too)?
With LAA, windowing hard on Tera helps you to cut out the volume better seeing the LT Atrium.
For a Post Op, the 2 snapshots on Tera that you have to take (when protocol requires it) are the same as visage?

What is the main difference between a Pre-Op and a Post-Op LAA?

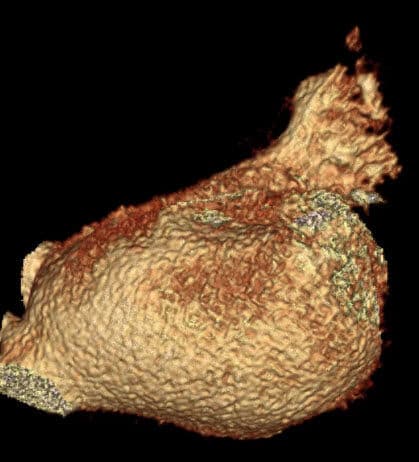
With a Pre-op LAA what does closing off the LAA prevent?

All appendages are alike.

Instead of hitting hollow view, what do you click to get this view on tera?

The facility will always call it a Watchman's or Amulet device.

When doing a LAA MPR, use the best window that lays out: Coronal or Axial
LAAs are positioned in AP unlike EPs which are PA.
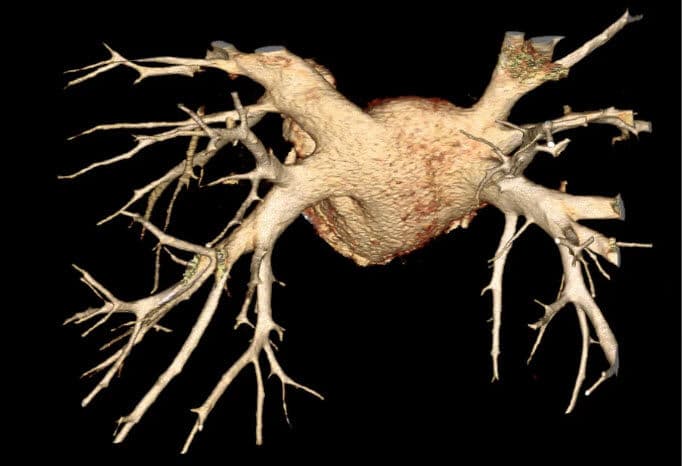
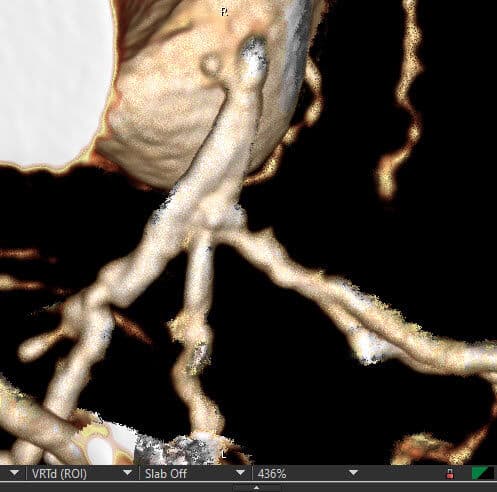
What are all the vessels of a CCTA that you have to CPR?

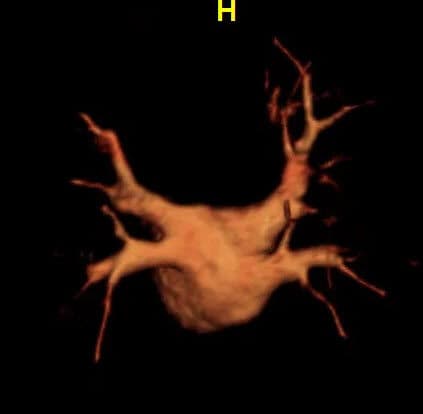
What part of the heart are you looking at for an EP?

For an LAA, do you have to have the PV branches on the volume?

What does a Triple Rule Out cover?

You cut off the heart for the volume spin on a Pediatric Chest?

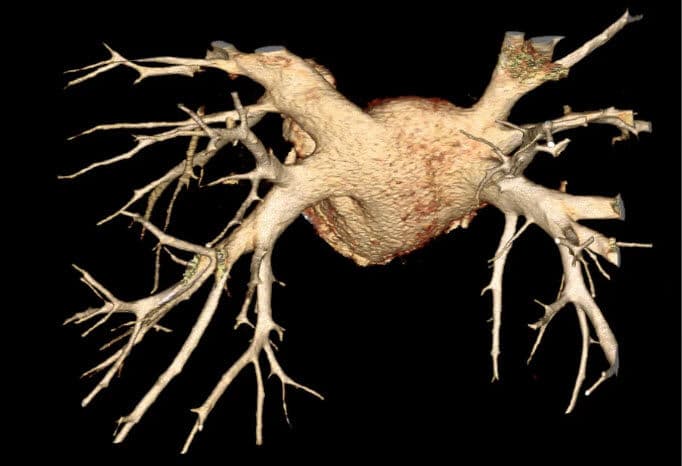
On a Pediatric Chest, you have to CPR the pulmonary artery each time.

Do they send contrasted data set for Pacemaker Leads?

What else is a Pre-Robotic Heart sometimes called?
What are the common reason(s) as to why a pre-robotic heart surgery is performed?

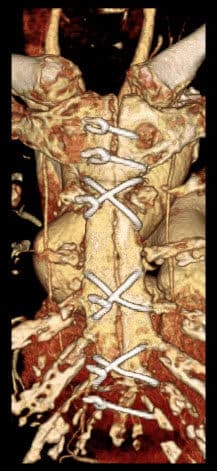
What does CABG stand for?

You have to cut for a CABG Re-do.
What does LIMA and RIMA stand for?

What are all the protocols we have learned so far?
What does CFA stand for?
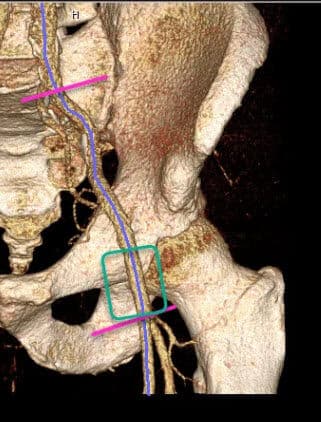
What landmark do you use to find the CFA?

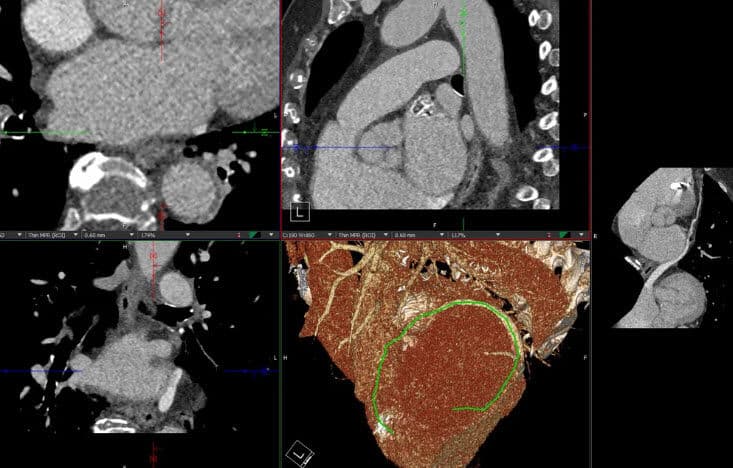
What is this called?
What are a few histories associated with a Pediatric Chest?

What is the groove that separates the ventricles?

What is the groove that separates the atriums from the ventricles?

Match the abbreviation with the full length name.
You can have a PLA come off the LAD.

How do we name a graft that isn't a LIMA or RIMA? What is the determining factor for naming these?
What vessel is between the true trifurcation of the LAD and CX?

When should you do an additional CPR on a CCTA?

A Ramus is always a Ramus no matter where it lands.
Diagonals can only come off _________.

What vessels can only have dual names?

What is the default increments for MPRs?

Do you include the LIMA/RIMA in the MPRs if they have grafts.

What do you line up with for this measurement?

What is this view called?
You will always have a left common (LCPV).

There can be a right common (RCPV).

How many ROI's do you have to have for this series?
Typically a function does not output over____%.

What are typical systolic phases?
You need to check all phases when editing a CFA.
A person with 40% or less cardiac output is considered in heart failure.
A person with normal cardiac output is ________.
It is important to be able to evaluate and estimate how much blood is being squeezed out to compare it to the result that the software provides for a CFA.
CFAs can be processed on Visage, Tera and Vitrea.
What is the max number of phases to load for a CFA?
You have loaded 0-100% phases on visage, it is out of order, what can you try to do to fix this?
The images below come in... should you add on a CFA?
Can you order a CFA on the images below?

The facility mentions they the want the RT ventricle evaluated with the LT ventricle. What protocol do you add?
You need to include the LVOT when editing but avoid adding the cusps.
What does LVOT mean?
You can leave your crosshairs on when doing gates.
If a facility sends CCTA images and the percentages range from 20-70%. What can you add?
If the facility sends Non-Contrasted images, can you add on a CA Score?
If the facility does not know the ethnicity for a CA Score, what do you default too?
